Update: Year marks big changes for states in administering and funding Medicaid
Note: This article was written in December 2025. The overview of new state laws and legislative proposals (see bottom of page) will be updated throughout 2026.
Nebraska is the first U.S. state to implement provisions in a 2025 federal law that mark one of the biggest changes in the 61-year history of Medicaid: requiring some enrollees to participate in work-related activities. Across the country, minus a state securing a “good faith” extension waiver, these work requirements must take effect in January 2027.
 They apply to the public health insurance program’s “expansion population” — low-income, able-bodied adults between the ages of 19 and 64. They also mean new obligations for states.
They apply to the public health insurance program’s “expansion population” — low-income, able-bodied adults between the ages of 19 and 64. They also mean new obligations for states.
And in the not-so-distant future, there will be added fiscal responsibilities and restraints for states under the federal law (HR 1 of 2025), especially among the 40 that have expanded Medicaid eligibility. For example, many states have come to rely on provider taxes to help finance their share of Medicaid; federal constraints on this revenue source either have taken effect or will do so soon.
“HR 1 is going to require action, much sooner than later, even if some of these provisions don’t take effect for a while,” says Edwin Park, a research professor at the Georgetown University McCourt School of Public Policy’s Center for Children and Families. “[States] can’t just wait until the last second to think how to deal with some of the federal revenue or the taxes going away or some of the implementation costs. They’re going to have to think now about what their revenues and spending look like over time.”
Big shift: Trends in Medicaid eligibility and spending
Nationwide, the number of people eligible for Medicaid has increased considerably over the past decade and a half as the result of actions taken by state legislators, governors and/or voters. Since congressional passage of the Affordable Care Act in 2010, states have had the option of extending Medicaid coverage to non-disabled adults with incomes of up to 138 percent of the federal poverty level and getting an enhanced federal funding match (currently 90 percent).
Most states have taken up the federal government on this offer.
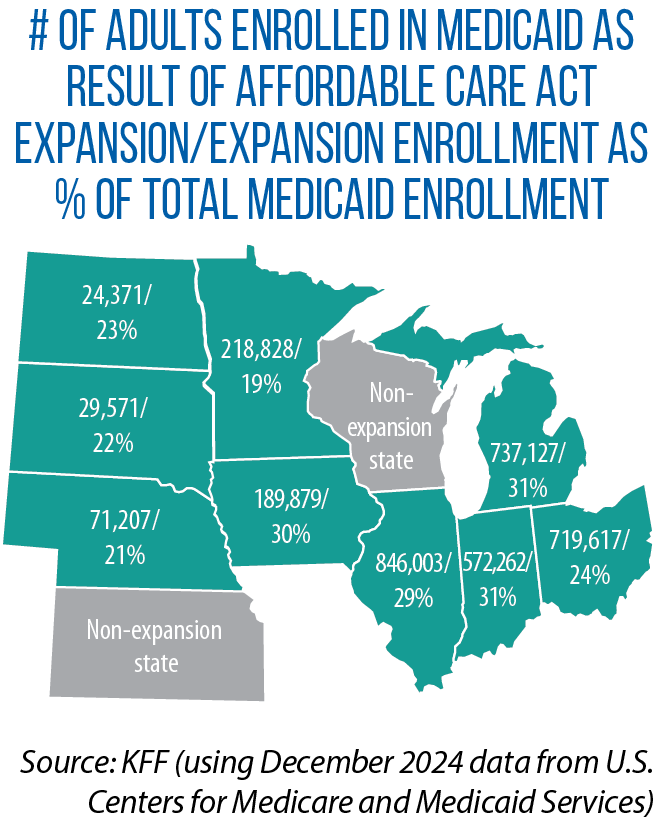
In the Midwest, Medicaid expansion is now a decade or more old in Illinois, Indiana, Iowa, Michigan, Minnesota, North Dakota and Ohio. The expansions in Nebraska and South Dakota are more recent; they also were the result of voter-approved ballot measures rather than legislative action.
In Illinois, Rep. Anna Moeller says, uninsured rates fell 44 percent and hospitals saw a 37 percent reduction in uncompensated care immediately after the change in her state. Across all 50 states, the expansion population now makes up about one-quarter of all Medicaid enrollees, KFF data show (see map above for percentages for the Midwest). In 2024, one in five Americans reported getting health insurance through Medicaid.
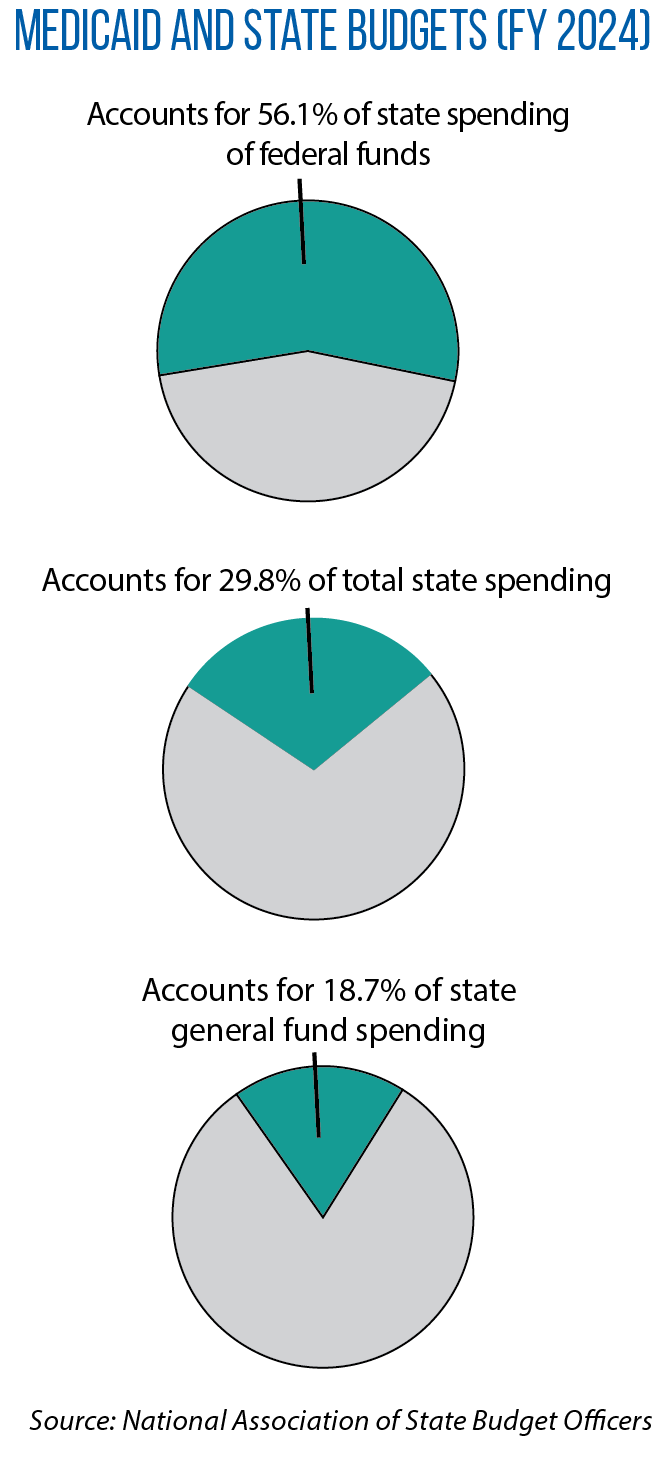
According to the National Association of State Budget Officers, as of fiscal year 2024, 30 percent of state spending — states’ own dollars, plus federal revenue — was on Medicaid; that compares to 22 percent in FY 2010, prior to expansions under the Affordable Care Act.
HR 1 has the potential of changing these numbers and trends.
New era: Details on Medicaid work requirements
 With the exceptions of Kansas and Wisconsin, all Midwestern states have adopted the Medicaid expansion. They must administer the new federal work requirements starting by early 2027. (Wisconsin also may have to comply because of coverage it provides via a federal waiver.) In an announcement of Nebraska’s first-in-the-nation implementation of this requirement, Steve Corsi, CEO of the state Department of Health and Human Services, hailed the change as a way of “encouraging greater economic and social participation.”
With the exceptions of Kansas and Wisconsin, all Midwestern states have adopted the Medicaid expansion. They must administer the new federal work requirements starting by early 2027. (Wisconsin also may have to comply because of coverage it provides via a federal waiver.) In an announcement of Nebraska’s first-in-the-nation implementation of this requirement, Steve Corsi, CEO of the state Department of Health and Human Services, hailed the change as a way of “encouraging greater economic and social participation.”
“Employment provides financial stability, fosters personal growth, and will help Nebraska’s small businesses in need of workers,” he said.
Similar sentiments, along with concerns about rising Medicaid costs, led some state legislatures to approve work requirements prior to enactment of HR 1. That includes Indiana (SB 2 of 2025), Iowa (SF 615 of 2025) and Ohio (HB 33 of 2023). South Dakota voters approved a ballot measure in 2024.
Actual implementation, however, will be new to all states in this region.
Outside the Midwest, a few states have carried out their own Medicaid work requirements, and those experiences point to a big challenge ahead: enforcing the federal rules while minimizing coverage losses among Medicaid-eligible individuals in the expansion population. In Arkansas, Park says, “people who should have been exempted from the work requirement or who met the work requirement” still lost coverage due to obstacles in reporting and documenting eligibility. In Georgia, “most of the lower-than-expected enrollment [in a Medicaid expansion] has been attributed to red tape associated with the work requirements,” he says.
Many exemptions, eligibility pathways in federal law
Under HR 1, individuals in the expansion population must show they have worked 80 hours per month or, alternatively, have participated in job training, education programs or community service. States must verify compliance when an individual applies for Medicaid, as well as redetermine eligibility at least once every six months. The federal law provides a host of exemptions from this work requirement — for those who are medically frail, disabled veterans, pregnant women, parents and guardians of children up to age 13, caregivers for disabled individuals, recently incarcerated individuals, and people receiving treatment for a substance-use disorder.
States also can provide a “short-term hardship exception” to residents of high-unemployment counties (a jobless rate of 8 percent or more or 1.5 times the national average).
“We know from data analysis that most individuals subject to the work requirements may already be working or may be eligible for some type of exemption,” notes Robin Rudowitz, vice president at KFF and director of its Program on Medicaid and the Uninsured.
KFF found that, as of 2023, nearly two-thirds of Medicaid-covered adults between the ages of 19 and 64 were working. Among those not working, nearly three in 10 qualified for an exemption.
On paper, then, work requirements will be met or not apply to most individuals in the expansion population. However, the paperwork — the need for documentation and verification — can keep individuals from being enrolled in or remaining on Medicaid.
In Illinois, state health officials have told legislators that anywhere from 270,000 to 500,000 people in the state will lose Medicaid coverage as a result of the work requirements.

Rep. Anna Moeller
On the high side of the estimate, “that’s about 15 percent of current enrollees,” says Moeller, who is chair of the Illinois House Medicaid Subcommittee and co-chair of The Council of State Governments’ Midwestern Legislative Conference Health & Human Services Committee.
“Just because people lose access doesn’t mean they stop getting sick; those costs get shifted to hospitals and emergency rooms and clinics,” she says. “Somebody has to end up paying for that care.”
Heavy implementation lift
Implementation of the work requirements, along with other rules related to compliance and more frequent checks on eligibility, is adding significant administrative burdens in Illinois, Moeller says. That includes a buildup of staff capacity, more communication and training with local partners, and upgrades in information technology. As part of HR 1, $200 million is available for states to establish systems around the new work requirements.
“To the extent that states can make it easy for people, and do things like data matching and not make individuals produce documentation, that certainly will be helpful in maintaining coverage,” Rudowitz says.
 With data matching, states can automate at least the redetermination and renewal process. Information from other state benefit programs or workforce databases are accessed and eligibility proceeds ex parte, meaning enrollees don’t need to provide documentation or fill out forms.
With data matching, states can automate at least the redetermination and renewal process. Information from other state benefit programs or workforce databases are accessed and eligibility proceeds ex parte, meaning enrollees don’t need to provide documentation or fill out forms.
“There are a lot of system changes that need to happen to do that data matching,” Rudowitz says. “No states are really set up right now to meet the new requirements. It’s a challenge of systems, timing, lack of guidance, staff capacity, all of these things.
“So even in those states that want to make it easy or want to be able to maintain coverage, there will be challenges in getting their systems and processes up to date.”
In an analysis for the first three months of 2025, Georgetown University researchers reviewed the share of renewals done ex parte in all states; percentages in the Midwest ranged from highs of 81.9 percent and 72.6 percent in Ohio and Minnesota, respectively, to lows of 17.2 percent and 17.3 percent in South Dakota and Nebraska, respectively.
Minnesota in recent years partnered with Code for America to improve the ex parte renewal process among aged, blind and disabled Medicaid enrollees. The result, according to Code for America, was a significant reduction in caseworker time as well as enrollees being renewed without having to take any action.
“If a state is wanting to reduce the enrollment loss that otherwise would happen, you certainly want to make the system as automated as possible, with as little burden as possible on individuals and families,” Park says. He adds, though, that provisions in HR 1 might point states “in the opposite direction of that approach.” Starting in October 2029, penalties will be imposed on states for erroneous payments or overpayments. The penalties apply to states with an error rate exceeding 3 percent.
“If you’re a state looking ahead, you will want to be designing systems that minimize what the federal government perceives to be an eligibility error,” Park says.
New fiscal restraints
As HR 1 advanced through the U.S. Congress, one option considered, but not ultimately included, was to end the enhanced federal matching rate of 90 percent for the Affordable Care Act expansion. (The traditional federal match ranges from 50 percent to 77 percent, according to KFF.) The enhanced match has made Medicaid expansion more fiscally (and politically) feasible in many states.
 States, too, have “trigger laws” that tie continuation of the Medicaid expansion to the enhanced rate. Ohio included such a trigger in its latest budget (HB 96 of 2025). According to Georgetown’s Center for Children and Families, three other Midwestern states have these trigger laws. Statutory language in Illinois and Indiana would end the expansion; Iowa’s trigger provision provides “more flexibility” on the state response. South Dakotans will vote on a trigger law in November.
States, too, have “trigger laws” that tie continuation of the Medicaid expansion to the enhanced rate. Ohio included such a trigger in its latest budget (HB 96 of 2025). According to Georgetown’s Center for Children and Families, three other Midwestern states have these trigger laws. Statutory language in Illinois and Indiana would end the expansion; Iowa’s trigger provision provides “more flexibility” on the state response. South Dakotans will vote on a trigger law in November.
One sure new fiscal restraint coming to states under HR 1 is new limits on the use of provider taxes.
“Even though they are restrictions on state behavior,” Park explains, “they produce savings [for the federal government] because the assumption is that states aren’t going to be able to replace those lost revenues.”
If a state spends less on Medicaid, the federal government has less to match.
Every state but Alaska imposes at least one of these provider taxes on hospitals, nursing homes, intermediate care facilities for individuals with disabilities, and/or managed-care organizations, according to the National Association of State Medicaid Directors. Nationwide, provider taxes account for about 18 percent of the non-federal share of state Medicaid spending. State general funds make up nearly all of the remaining non-federal share, according to KFF.
Under HR 1, states cannot establish new provider taxes or increase the rates of existing ones. These restrictions cover all states, regardless of whether they expanded Medicaid.
“It’s hard to assess the impact because we don’t know what states may have moved forward with more provider taxes” if they had been allowed to do so, Rudowitz says.
But past practice in many states has been to raise or expand provider taxes during economic downturns, she says, as a means of maintaining Medicaid coverage and provider payments when state budgets are under duress and the availability of state general funds is limited. This option no longer exists.
Park notes, too, that provider taxes have been used by some states to expand their Medicaid programs.
Shrinking provider taxes
Another piece of HR 1 applies only to the Medicaid expansion states’ use of provider taxes. For those states, the federal government will phase in stricter limits on what’s known as the “safe harbor threshold.”
“Safe harbor” refers to states being able to get a federal match of Medicaid dollars from revenue generated by the provider tax. Right now, the tax threshold is 6 percent of a provider’s net patient revenue. In expansion states, though, that threshold declines by half of a percentage point in each fiscal year starting in FY 2028 before reaching 3.5 percent in FY 2032. (Provider taxes on nursing homes and intermediate care facilities are exempt.)
A KFF analysis shows that seven Medicaid expansion states in the Midwest — Illinois, Indiana, Iowa, Michigan, Minnesota, Nebraska and Ohio — impose a provider tax on hospitals exceeding that 3.5 percent threshold. An Illinois provider tax on managed care organizations also is higher than 3.5 percent.
“There’s a little bit of a lag on when these provisions go into effect,” Rudowitz says, “but this is going to be a big issue for state budgets.”
In Illinois, legislators have been told that HR 1 will result in a cumulative loss of $6.6 billion between FY 2028 and 2031 due to mandatory cutbacks in the provider tax and reduced federal support.
The federal changes are coming after a period in which many states moved ahead not only with the Medicaid expansion, but other policies to enhance benefits or boost access to behavioral health and various long-term-care options, Rudowitz says.
She adds that “states already have been facing a lot of cost pressures on the Medicaid side — pressures to increase provider rates, address inflation and workforce challenges.”
One area to watch in particular is state funding of home health care, Rudowitz says. Home- and community-based services account for a large portion of Medicaid spending, but providing these services is optional.
“They are expensive services, and they’re not required by the [federal] statute,” she says. “So we could see states wind up having to ratchet back or make changes to some of these home health care programs. And that could affect people who need the care or the payments to the providers.”
In support of its work on behalf of The Council of State Governments’ Midwestern Legislative Conference Health & Human Services Committee, CSG Midwest has developed two analyses on the impacts of HR 1 on the 11 states in the Midwest, with a particular focus on direct fiscal effects in two safety-net programs: Medicaid and the Supplemental Nutrition Assistance Program, or SNAP. This analysis on HR 1 and Medicaid was produced in December 2025. The first analysis was released in July 2025 and focuses on changes that will affect state administration and funding of SNAP. It can be found here.
Movement on Medicaid proposals: Overview of legislative activity in 2026 (as of May)
Illinois: Loan program for distressed hospitals; $55 million for more staff and system upgrades
Illinois lawmakers approved a budget for fiscal year 2027 that includes provisions to help healthcare providers likely to be impacted by federal changes under HR 1 and to prepare the state’s overall health care system.
One new policy of note: Under the new budget, in tandem with separate legislation (SB 3365), Illinois is establishing the $85 million Distressed Hospital Loan Program, which will provide interest-free loans in order to prevent the closure of hospitals or to facilitate reopenings. To secure a loan, a hospital must submit information that demonstrates its need for “bridge financing” and that lays out a plan “to regain financial viability.” It must develop an emergency and financial contingency plan and provide additional financial transparency.
Among the hospitals likely to have access to the new loan program: those serving a disproportionate share of uninsured and Medicaid patients and/or those providing care in underserved rural or urban areas of the state. (As this Chicago Tribune article notes, the new loan program will replace the state’s use of “advanced payments” to assist these hospitals. The change provides more accountability and financial safeguards, legislators say.)
Illinois’ FY 2027 budget also provides additional state-based funding for federally qualified health centers: nonprofit health centers or clinics that serve medically underserved areas and populations and that provide care regardless of one’s ability to pay. A total of $50 million is provided to these centers to allow for increased payment system rates. (The amount provided in FY 2026 was $40 million.)
Another part of the budget details the state’s allocation of $118 million to provide “add-on” payments to safety-net hospitals: facilities that serve a significantly high number of uninsured and low-income patients.
Lastly, lawmakers are investing $55 million to hire 450 additional staff and to update eligibility-determination systems. State officials say this appropriation is needed to comply with federal changes (in HR 1 of 2025) regarding eligibility and work requirements for Medicaid and the Supplemental Nutrition Assistance Program (SNAP).
Indiana: Medicaid payment reform approved; plus details on this year's SB 1
New structure for hospital payments
Indiana secured federal approval in May for a plan that restructures state Medicaid payments to hospitals and aims to promote affordability across the broader health care market. State officials also say the plan will boost funding for hospitals, including those in rural areas, that “already charge lower prices but operate on tight margins.”
The State Directed Payment initiative is tying Medicaid reimbursement for hospitals to the commercial prices they charge — those with lower commercial prices (based on their average commercial rate, or ACR) receive a larger Medicaid funding increase; those with higher prices receive smaller Medicaid funding increases.
Indiana hospitals are classified into one of four classes, or tiers. Critical access hospitals and public rural hospitals make up one of these tiers; they will receive the largest increase in Medicaid funding, a 158 percent increase over current fee schedules. The increases for other hospitals range between 120 percent and 155 percent, depending on their commercial pricing.
The plan also modernizes Indiana’s Hospital Assessment Fee structure in order to bring more federal Medicaid dollars to the state.
SB 1 will guide implementation of new federal law
Indiana’s SB 1, signed into law in March, codifies state implementation of the 2025 federal law (HR 1) while, in some cases, setting more stringent rules than required — for example, requiring redeterminations every six months for some Medicaid recipients outside the expansion population, establishing a three-month “look back” and documentation requirement (HR 1 requires a “look back” of one, two or three months), and providing fewer short-term exemptions from the Medicaid work requirement.
The bill also establishes the Indiana Rural Health Transformation Fund, along with funding allotments and a process for legislative review.
Here is a summary of some of the provisions in SB 1:
• Require Medicaid eligibility redetermination at least one time every six months for a nonelderly adult Medicaid recipient whose eligibility is based on income. (A redetermination must be made at least one time every 12 months for other Medicaid recipients)
• Prevent Medicaid enrollment in more than one state by transmitting information to the U.S. Department of Health and Human Services.
• Count any income of a household member who is ineligible due to the household member’s immigration status when determining Medicaid eligibility.
• Establish new work requirements.
• Require documentation by individuals in the Medicaid expansion population that shows compliance with work requirements over three consecutive months.
Iowa: Higher tax on insurers
One policy strategy in Iowa to address the state’s Medicaid budget shortfall is a raise in the tax imposed on health maintenance organizations (HMOs).
Signed into law in March, HF 2739 increases the state HMO tax on premiums — from a previous rate of 0.925 percent to 3.5 percent, effective from the start of 2026 through Sept. 30, 2026. The tax rate will then be set at .95 percent starting on Oct. 1. The temporary increase to 3.5 percent is contingent on federal approval, the Iowa Legislative Service Agency Fiscal Services Division notes in its summary of HF 2739.
“Total revenue available to Medicaid is estimated to increase by approximately $6.6 million in FY 2026, $165.2 million in FY 2027, and $16.4 million in FY 2028, including increased payments to the Medicaid MCOs, due to the increased taxes on the MCOs,” the LSA notes.
Kansas: New law requires changes in Medicaid administration
Sub HB 2731 passed the Legislature in March and was vetoed by Gov. Laura Kelly. A day after her veto, the House and Senate successfully overrode it.
Among the provisions:
- Require data matching among state agencies to check for changes in circumstances that may affect eligibility. The legislation details the types of data matching that must occur and the frequency (monthly checks of death and incarceration records, potential changes in residency, and lottery winnings; quarterly checks of employment and wages).
- Prohibit agencies during the enrollment process from accepting self-attestation (without agency verification) of income, residency, age, household composition and other factors that impact program eligibility.
- Limit retroactive eligibility in Medicaid and other public assistance programs to two months.
- Require legislative approval of any geographic or work requirement waivers to public assistance programs.
- Submit monthly data-matching reports on Medicaid enrollees to the federal government to prevent enrollment in multiple states.
In a message explaining her veto (subsequently overridden by the Legislature), Gov. Laura Kelly said the law “adds unnecessary costs and bureaucracy in our human service and health agencies.” She pegged the cost at nearly $4 million, and said the measure will likely cause an increase in the state’s processing error rate and result in federal monetary penalties.
“[Our] agencies already exchange data with each other and engage in rigorous oversight to reduce fraud and ensure that only eligible persons receive public assistance and health benefits,” she said.
Another provision in Sub. HB 2731 calls on the Kansas Department for Aging and Disability Services to seek federal approval of a policy to establish continuous Medicaid eligibility protections for individuals who have a documented, permanent intellectual or developmental disability and are receiving services through a Home and Community Based Services waiver.
Michigan: Workforce investments tied to HR 1
In Michigan, where partisan control of the Legislature is split, the final budget for FY 2027 ultimately received overwhelming support in the House and Senate. Passed by the Legislature in early July, SB 878 has several new Medicaid policies and expenditures related to the federal changes under HR 1.
Apprenticeships, community health navigators and more
In response to HR 1’s new work requirements for Medicaid and the Supplemental Nutrition Assistance Program (SNAP), lawmakers included a $54.3 million line item ($14.7 million federal/$40 million own-state revenue) to increase staffing capacity, administrative supports and oversight. The hiring of an additional 421 limited-term, full-time-equivalent employees is authorized in the budget.
Michigan also is investing in initiatives to help individuals meet the work requirements, as well as navigate new federal rules on eligibility.
For example, a total of $4 million will be used to increase opportunities for people to participate in registered apprenticeship programs. Such participation fulfills the work requirement. Another $10 million will go to Michigan Works! offices across the state providing services related to job searches, readiness, and placements; skills and vocational training; and pre-apprenticeship activities.
In all, Michigan Gov. Gretchen Whitmer says, the state is making $31.5 million in workforce investments to help Michigan residents maintain access to Medicaid and SNAP.
The state also is putting $20 million toward the work of “community health navigators,” organizations that assist individuals with securing or maintaining Medicaid coverage and SNAP assistance.
Early in 2026, the governor proposed a series of new revenue generators to support the state’s Medicaid program — for example, a rise in the tobacco tax, new excise taxes on vaping products and digital advertising revenue, and new taxes on casinos and sports betting.
The final version of SB 878 does not include these proposals.
According to Whitmer, though, the budget does include an $185 million plan to stabilize Medicaid funding “through efficiency savings identified in collaboration with stakeholders to address costs, increase accountability and align resource effectiveness while maintaining sustainability of services.”
More legislative oversight, plus more eligibility verification
The Michigan Legislature must now give the OK before the governor and executive branch pursue U.S. Centers for Medicare & Medicaid Services waivers or Medicaid State Plan Amendments. Statutory approval by lawmakers is required.
SB 878 also sets out rules on Medicaid eligibility and verification.
The state will not allow for “self attestation” as part of the process for determining Medicaid eligibility; specifically prohibited is unverified, self reporting by individuals of their income, residency, identity, household composition, and citizenship or immigration status.
Additionally, the Michigan Department of Health and Human Services must verify application information through a review of data available from state and federal agencies (ex parte verification).
The department also must regularly conduct state and federal matches to ensure Medicaid participants are eligible. As part of these reviews, ineligible participants will be identified and removed from the Medicaid program.
Quarterly reports from the department will detail: 1) the data sources it used to verify eligibility; 2) the number of people found to be ineligible for Medicaid as the result of its reviews; 3) and the impacts of HR 1 on eligibility.
Minnesota: New laws to combat fraud, stabilize at-risk hospitals
t the end of their 2026 session, Minnesota legislators passed bipartisan bills providing greater oversight of the Medicaid program, including more staff and new tools for fraud investigations.
Additionally, parts of an omnibus measure signed into law in May aim to help hospitals impacted by reductions in federal Medicaid dollars and address state compliance with HR 1.
Combating fraud
SF 856 creates a new independent Office of the Inspector General to ensure “accountability, transparency, and integrity in the operations of state executive branch agencies and programs.”
One function of this office is to provide another layer of protection against Medicaid fraud and abuse.
Investigations still remain the responsibility of the Minnesota Department of Human Services and a Medicaid Fraud Control Unit within the attorney general’s office. However, the inspector general (who will be appointed by the governor, with consent of three-fifths of the Minnesota Senate) will have the authority to conduct independent investigations.
Additionally, more funding for the attorney general office’s Medicaid Fraud Control Unit will allow for the hiring of more investigators and prosecutors. This appropriation is part of SF 4612, passed by the Legislature in May.
Minnesota Attorney General Keith Ellison notes that the work of this Fraud Control Unit also will be strengthened by other statutory changes in SF 4612:
- expanding the definitions of Medicaid fraud,
- enhancing sentencing in high-dollar cases,
- adding Medicaid fraud to Minnesota’s racketeering statute,
- increasing the state’s ability to recover tax dollars lost to fraud, and
- providing the unit with the authority to subpoena financial records during criminal Medicaid fraud investigations.
Changes in Medicaid policy
SF 4612 is an omnibus bill that includes several policy and administrative changes to Minnesota’s Medicaid program.
For example, a new Health Care Eligibility Oversight Unit will be established within the state Department of Human Services “to ensure federal and state Medicaid eligibility requirements are consistently applied by all processing entities.” A central goal is to decrease eligibility errors. (In Minnesota, Medicaid and many other public assistance programs are county-administered.)
Rep. Joe Schomacker, a key negotiator of the omnibus bill, says the new law will strengthen Medicaid program integrity “by expanding provider enrollment and revalidation requirements, increasing oversight of high-risk providers, allowing stronger prepayment and post-payment reviews, and giving the Department of Human Services clearer authority to suspend billing privileges when necessary to protect public funds.”
To help hospitals being impacted the most by reductions in federal Medicaid dollars under HR 1, the Legislature is creating a onetime, $30 million Hospital Stabilization Program — “financial relief to support critical access hospitals, rural emergency hospitals, and hospitals that provide a disproportionate level of uncompensated care.”
Additionally, Hennepin Healthcare will receive a one-time $205 million emergency stabilization grant, with up to $500 million available through 2031. The Minnesota Medical Association notes that Hennepin Healthcare is projected to lose approximately $50 million this year, with deficits potentially reaching $1.7 billion over the next decade, as the result of changes in federal policy.
According to Minnesota Sen. Melissa Wiklund (like Rep. Schomacker, a key legislative negotiator on SF 4612), the omnibus bill has two key provisions regarding state implementation of HR 1 and Medicaid:
1) Statutory language and the allocation of state funding to preserve three-month retroactive coverage for all enrollees for one additional year (through Jan. 1, 2028); and
2) Greater flexibility for the Department of Human Services “to interpret federal work requirement rules in ways that help prevent Minnesotans from unnecessarily losing coverage.”
She also highlighted the value of investing more in the Medicaid Fraud Control Unit. That investment unlocks a “3:1 funding match from the federal government,” Wiklund says.
Proposals to revamp payment and delivery models
At the start of the year, Minnesota Gov. Tim Walz proposed an overhaul of the state’s Medicaid payment and service delivery model: eliminate the use of private insurers (managed care organizations) and move to a system of direct state payments to medical providers.
Bills reflecting this change were introduced in the Minnesota Legislature: SF 3612 and HF 3476, with proponents citing cost savings from such a shift in Connecticut. Like-minded proposals have been introduced in 2026 in Ohio and Wisconsin.
Gov. Walz’s policy framework also included shifting eligibility determinations from Minnesota counties to the state. The proposals did not advance prior to the close of Minnesota’s legislative session.
Nebraska: Questions over retroactive Medicaid eligibility
In early 2026, Nebraska Gov. Jim Pillen unveiled a series of mid-biennium budget adjustments, some of which impact the state Medicaid program.
• Lower Medicaid costs related to cost-sharing options, such as premiums and copayments for certain conditions and services for adults, in order to promote healthier lifestyles.
• Eliminate retroactive Medicaid eligibility.
• Adjusting state Medicaid rates and rate-setting structures for providers (including those providing Applied Behavior Analysis, or ABA, therapy) to reduce costs.
In contrast to the governor’s proposed elimination of retroactive Medicaid eligibility, legislation was introduced (LB 777) requiring the state to provide the maximum of federally allowable retroactive coverage eligibility for Medicaid. (The maximum under federal law is one month for the Medicaid expansion population and two months for other enrollees.)
This policy was included in a separate measure (LB 958) that passed near the end of Nebraska’s 2026 legislative session with near-unanimous support.
According to Unicameral Update, along with the state guaranteeing the maximum amount of allowable retroactive coverage under the 2025 federal law, LB 958 requires future annual agency reports on Medicaid and long-term care to include information on the program’s work requirements. That includes the number of people denied coverage or renewal for not meeting the requirements, as well as the number of exemptions allowed.
Additionally, legislators are requiring these agency reports to provide details on cost sharing, premiums, copays and deductibles in the Medicaid program, along with the number of identified cases of concurrent enrollment.
South Dakota: Higher payment rates for providers
South Dakota’s enacted budget for fiscal year 2027 (HB 1326) includes a 1.4 percent increase in the rates that the state will pay to Medicaid providers.
Additionally, in November 2026, South Dakotans will vote on a legislatively referred constitutional amendment (HJR 5001) calling for an end to the Medicaid expansion in South Dakota if the federal matching rate falls below 90 percent. Voters previously approved the Medicaid expansion.
Wisconsin: Extension of postpartum coverage
A new law in Wisconsin (SB 23) extends postpartum Medicaid coverage from 60 days to one year.